Categories
Information
On this page you will find helpful information about the joint systems and carbon springs from the Gottingen trading house. If you have further questions, you can of course contact us. To the contact form.
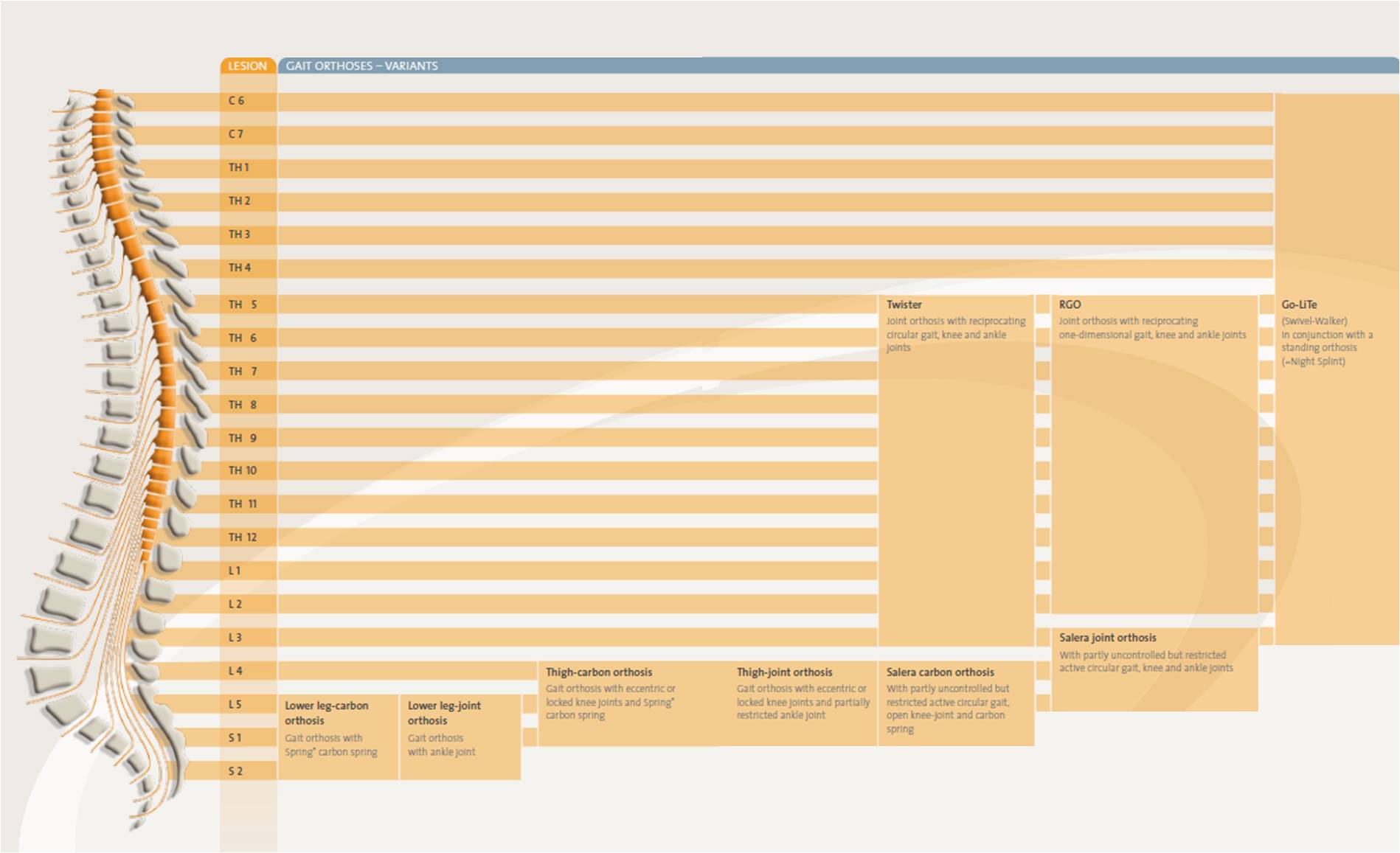
Depending on the lesion different joints can be installed in the orthotics. Overview:
HKAFO
The kinetic combinations of the two-axis and triaxial hip joint systems make circular gait possible. The pelvis endeavours to execute a rotation around its own vertical axis. We call this circumduction. In the process, the leg describes an arc of a circle outwards around its turning centres in the pelvis (left/right hip joint). If this kinetic sequence is prevented from occurring, as with single-axis hip joints, the patient has to expend additional energy during the hip extension to lift his body weight or to rotate via orthotic shoe soles and the ground.
The left picture below shows Twister und Salera hip joints, allowing pelvic rotation. The right picture shows a single-axis joint, which halts after each step and is pushed on again with new energy.

The use of circumduction in pelvis-spanning orthoses systems makes energy-saving
walking possible and consequently promotes the acceptance of the orthosis.
Comparison commencing gait and double step
FIRST STEP
| TWISTER | RGO | SALERA |
|---|---|---|
| Both legs are parallel, and the walking aid must be adjusted so that the elbow joint is half extended in order to be able to shift the weight through an extension. | Both legs are parallel, and the walking aid must be adjusted so that the elbow joint is half extended in order to be able to shift the weight through an extension. | Both legs are parallel, and the walking aid must be adjusted so that the elbow joint is bent at approx. 75 %. The hip joints are in maximum flexion to the side. |
| Shifting weight onto a standing leg using the walking aid. A slight inclination to the side enables the leg that is not under pressure, the so-called free leg, to be lifted. By additionally extending the hip, the free leg is now brought forward. | Shifting weight onto a standing leg using the walking aid. A slight inclination to the side enables the leg that is not under pressure, the so-called free leg, to be lifted. By additionally extending the hip, the free leg is now brought forward. | Weight shifting onto a standing leg using the walking aid. The side inclination of the trunk onto the free leg side enables the free leg to be lifted through the abduction lock. This is supported by the still functioning quadratus lumborum muscle. |
| During the step, the hip joint of the free leg is carried forward from below. Both legs continue to stand in the direction of movement (the front leg in outward rotation, the back leg in inward rotation to the pelvis). | The pelvic section remains parallel to the legs during the step. In order to bring the free leg forward, the patient must either lift his body weight against the force of gravity during the hip extension, or rotate under increased friction between the sole of the shoe and the ground. | The simultaneous extension of the pelvis, favoured by the shifting of the force of gravity between foot and walking aid, brings the free leg forward. The leg in front is in outward rotation to the pelvis, the leg behind is in inward rotation to the pelvis. |
| In order for the free leg to become the standing leg, the centre of gravity is brought forward after the heel strike. | in order for the free leg to become the standing leg, the centre of gravity is brought forward after the heel strike. | In order for the free leg to become the standing leg, after the heel strike the centre of gravity is brought forward. |
| The walking aid is dragged along. | The walking aid is dragged along. | The walking aid is dragged along. |
SECOND STEP
| TWISTER | RGO | SALERA |
|---|---|---|
| The second step is initiated by putting pressure on the walking aid while simultaneously extending and inclining the hip to the side of the standing leg. | The second step is initiated by putting pressure on the walking aid while simultaneously extending and inclining the hip to the side of the standing leg. |
The second step is initiated by putting pressure on the walking aid while imultaneously extending and inclining the hip to the side of the standing leg. |
| The free leg comes forward from below by slightly inclining to the side and extending the hip following the centre of gravity. The position of the leg remains in the direction of movement (front leg changes to outward rotation, back leg to inward rotation to the pelvis). | In order to be able to bring the free leg forward, the patient must either lift his body weight against the force of gravity while extending the hip, or rotate between the sole of the orthotic shoe and the ground under increased friction. | A pelvic rotation leads the free leg side forward during the step. Both legs remain in the direction of movement. The knee bend during the back-swing is extended before the heel strike by the residual force of the quadratus lumborum muscle. |
| After the heel strike, the centre of gravity drifts forward. The free leg becomes the standing leg and the cycle begins again. | After the heel strike, the centre of gravity drifts forward. The free leg becomes the standing leg and the cycle begins again. | After the heel strike, the centre of gravity drifts forward. The free leg becomes the standing leg and the cycle begins again. |
| The Twister gait orthosis allows a circular gait in the step cycle. This can be summed up by saying that the energy expended on walking decreases through the feasible pelvic rotation and by avoiding the rotation between the ground and the soles of the orthotic shoe. These factors and the lower expenditure of force on initiating a step thus promote the acceptance of the orthotic device. Utilizing the entire kinetic swing of the pelvis counteracts contractures. | The Salera gait orthosis allows a circular gait in the step cycle. This can be summed up by saying that the energy expended on walking decreases through the feasible pelvic rotation and by avoiding the rotation between the ground and the soles of the orthotic shoe. These factors and the lower expenditure of force on initiating a step thus promote the acceptance of the orthotic device. Using the entire kinetic swing of the pelvis counteracts contractures. |